HNcorpsman
Forum Lieutenant
- 239
- 1
- 0
so i recently went through a class taught by a Dr. Hagmann, a retired COL in the army, he still is an emergency physician today...
anyways he was explaining the subject of C-spine, and how it has become such a big issue... he started off with a story of a paramedic. the paramedic came upon a PT who was shot in the jaw... upon arrival the pt was breathing and alert but had alot of bleeding from the jaw, he was also sitting up spitting onto the ground... so what are we trained to do when someone gets shot? C-spine... well he told the PT to lay down, once pT lays down he starts to choke and gag, eventually he stops breathing... he tries to get the PT to breath again using basic treatment, no good.. so he tries to intubate, no good, after several tries... so he does what he has to do and gives and emergency cric... he gets it. he then tries to control the bleeding, but wait the pT looks a little pale (shock) so then he gives the PT an IV and then the bleeding gets worse... because the IV the fluids raised his blood pressure (cause more bleeding) and diluted the blood... the PT eventually codes on the way to the hospital, and does not make it... all the medic had to do was control the bleeding.. the PT would have been still here today.
anyways the Dr. explained that in some years from now... they will probably
begin to "clear" c-spine in the field, and it will be the paramedics call.. this is what he explained
NO c-spine IF...
1. if no mechanism
a.falling on flat ground
b. gunshot wound
2. if no pain on range of motion
3.no tenderness,
4. no step offs
5. no numbness or tingling
C-spine if
1. axillary load (hitting top of head)
a.diving into swimming pool
b.ejecting out of plane
c.dropping hatch on head
2.traction load (pulling head)
a. hanging
b. parachuting
3. flexion/extension(whiplash)
a.car accident
b. ejected from vehicle
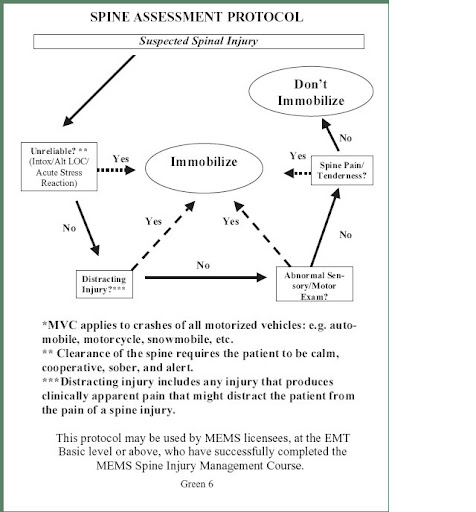
to clear c-spine ask these questions
1. was there a mechanism?
2.is there pain in the neck?
3.is there tenderness?
4. are there any step offs?
5. is there distal neuro? tingling?
6. is there pain in range of motion?
anyways he was explaining the subject of C-spine, and how it has become such a big issue... he started off with a story of a paramedic. the paramedic came upon a PT who was shot in the jaw... upon arrival the pt was breathing and alert but had alot of bleeding from the jaw, he was also sitting up spitting onto the ground... so what are we trained to do when someone gets shot? C-spine... well he told the PT to lay down, once pT lays down he starts to choke and gag, eventually he stops breathing... he tries to get the PT to breath again using basic treatment, no good.. so he tries to intubate, no good, after several tries... so he does what he has to do and gives and emergency cric... he gets it. he then tries to control the bleeding, but wait the pT looks a little pale (shock) so then he gives the PT an IV and then the bleeding gets worse... because the IV the fluids raised his blood pressure (cause more bleeding) and diluted the blood... the PT eventually codes on the way to the hospital, and does not make it... all the medic had to do was control the bleeding.. the PT would have been still here today.
anyways the Dr. explained that in some years from now... they will probably
begin to "clear" c-spine in the field, and it will be the paramedics call.. this is what he explained
NO c-spine IF...
1. if no mechanism
a.falling on flat ground
b. gunshot wound
2. if no pain on range of motion
3.no tenderness,
4. no step offs
5. no numbness or tingling
C-spine if
1. axillary load (hitting top of head)
a.diving into swimming pool
b.ejecting out of plane
c.dropping hatch on head
2.traction load (pulling head)
a. hanging
b. parachuting
3. flexion/extension(whiplash)
a.car accident
b. ejected from vehicle
to clear c-spine ask these questions
1. was there a mechanism?
2.is there pain in the neck?
3.is there tenderness?
4. are there any step offs?
5. is there distal neuro? tingling?
6. is there pain in range of motion?
Last edited by a moderator: