Been a heck of a week, I know this one's a little late. It's not as train wreckish as the last one, so I'm sure y'all will get it quick.
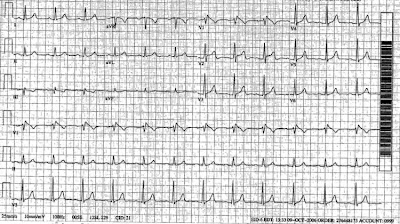
Dispatched to a 32 YOM c/o chest pain after a traumatic injury. Pt was playing hockey and took a hard hot against the boards.
You find a tall, thin male c/o left sided chest pain. You notice as you walk up he's pale "as a ghost". Go...
Dispatched to a 32 YOM c/o chest pain after a traumatic injury. Pt was playing hockey and took a hard hot against the boards.
You find a tall, thin male c/o left sided chest pain. You notice as you walk up he's pale "as a ghost". Go...