- 9,736
- 1,174
- 113
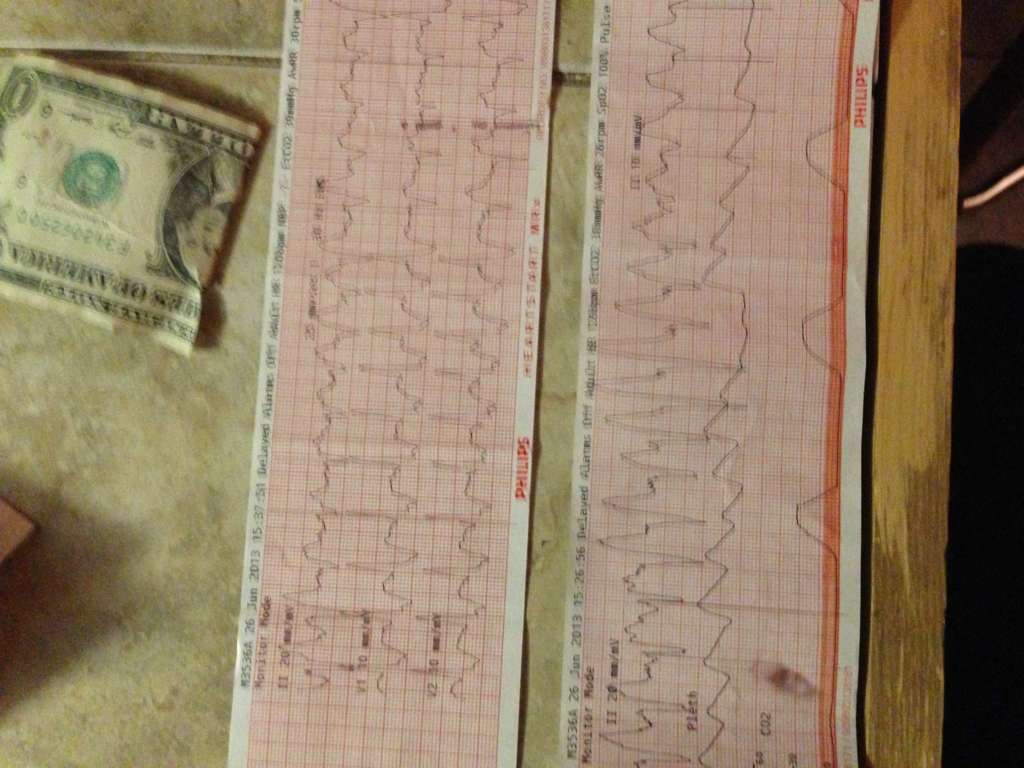
51 year old, trached, vent dependent male in an acute care SNF. Changing his shiley tube and he vomited and aspirated. Normally only on pressure support but they had to sedate him, suction the crap out of him and put him on SIMV to keep him saturating well.
Not really a scenario, more just looking for opinions on the rhythm. It was one of those calls that I didn't feel like I did well on. Nabbed the IV of a lifetime on the third attempt, 22g in the pointer finger between the first and second knuckles (proximal to distal) that flowed like a champion once I splinted that and the adjacent finger together with the help of a tongue depressor. Started 150 of amio over 10 minutes but were at the ER before it was finished, doc continued though so that made me feel a little more confident about my decisions.
Sorry the really good pictures got turned in with my chart but this is the leftovers, should've printed everything again.
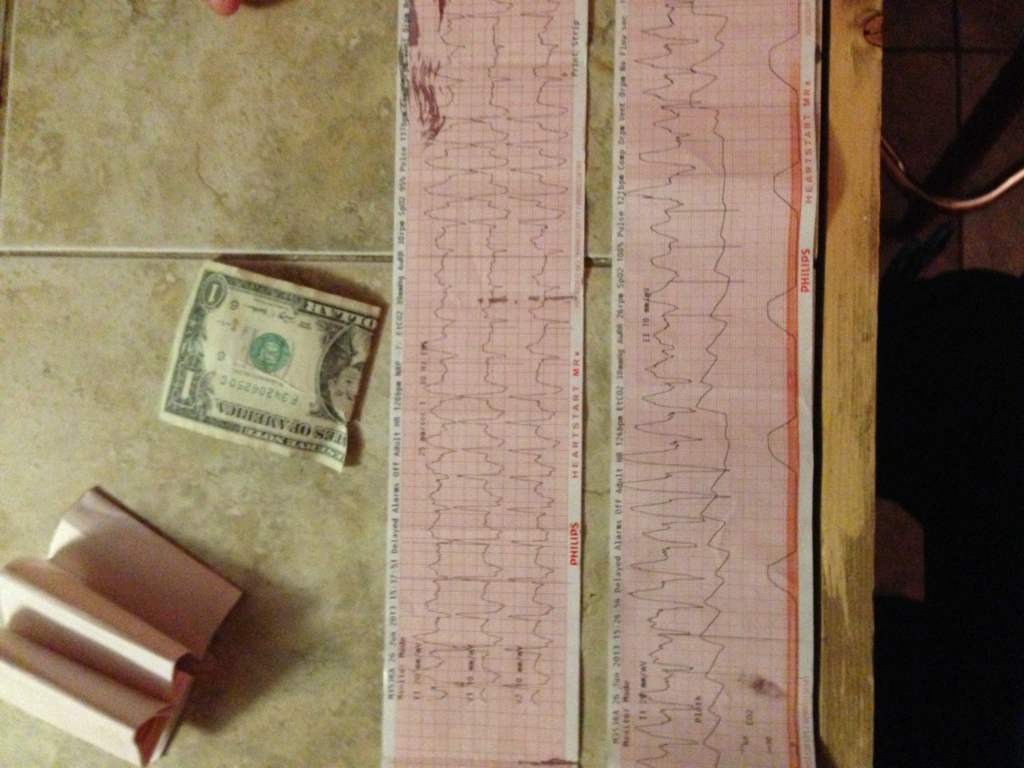
Not really a scenario, more just looking for opinions on the rhythm. It was one of those calls that I didn't feel like I did well on. Nabbed the IV of a lifetime on the third attempt, 22g in the pointer finger between the first and second knuckles (proximal to distal) that flowed like a champion once I splinted that and the adjacent finger together with the help of a tongue depressor. Started 150 of amio over 10 minutes but were at the ER before it was finished, doc continued though so that made me feel a little more confident about my decisions.
Sorry the really good pictures got turned in with my chart but this is the leftovers, should've printed everything again.