VFlutter
Flight Nurse
- 3,728
- 1,264
- 113
I have had a few days off and got bored so I figured I would write this up. I've had this conversation a few times lately and think that is useful knowledge. Just a few tips and tricks. There is very much an art along with the science of Rapid Infusion and Large Bore IVs.
For the sake of this discussion Large Bore refers to 14-16g IVs. Always consider what is going on with your patient; For those who truly need large volumes of fluid infused rapidly it can be a lifesaver however if done inappropriately it can very detrimental. Remember balanced resuscitation, permissive hypotension, hyperchloremic acidosis, and all that fun stuff.
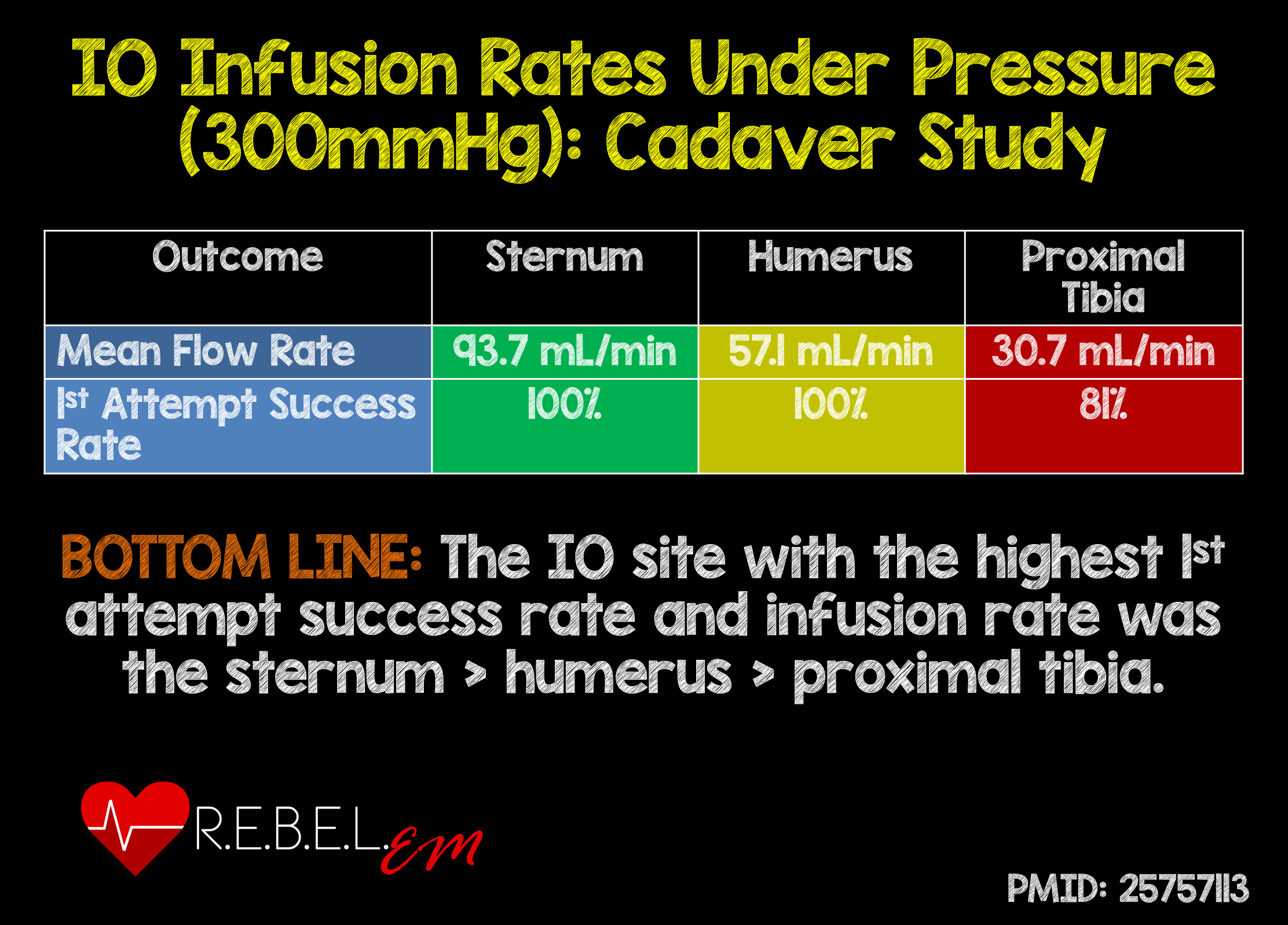
IV selection is extremely important when using rapid transfusion devices such as a Level One or Bellmont however is still important for EMS. A 14g with a pressure bag can infuse 1L of fluid is under 2 minutes. Also great for blood products. Depending on length some 14g catheters actually flow faster than a Cordis.

/https://lifeinthefastlane.com/ccc/device-flow-rates/
https://etmcourse.com/large-bore-iv-access-showdown/
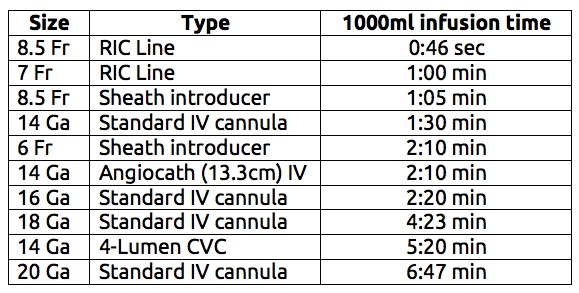
For large volume rapid infusion short/wide PIV catheters are best. As you can see from the chart length makes a big difference in IVs of the same gauge (Poiseuille's Law). IOs and CVC are great for medications but worthless for rapid infusion. Pressure bags or just squeezing the bag can increase flow rates substantially.
The biggest thing that many people do not realize is how much flow rates are decreased with needless connectors or extension sets. As much as 30-40% less. If you need high flow connect tubing directly to the catheter hub. It is hard to break the habit of instantly putting a saline lock and the IV you just placed.
If you only have the one IV and you are frequently pushing medications then a 3-way stopcock is a good compromise. Stopcocks will restrict flow slightly but much less than a needless connector. If you happen to see a stopcock with a yellow top then those are usually "High Flow" are will likely flow as fast as your IV will allow.
You can usually find these in the Cath Lab or with Anesthesia supplies.

So long story short Large Bore IVs are extremely useful when used appropriately. If you need high flow then go for a 14g or 16g, ditch the needless connector, and grab a pressure bag.
For the sake of this discussion Large Bore refers to 14-16g IVs. Always consider what is going on with your patient; For those who truly need large volumes of fluid infused rapidly it can be a lifesaver however if done inappropriately it can very detrimental. Remember balanced resuscitation, permissive hypotension, hyperchloremic acidosis, and all that fun stuff.
IV selection is extremely important when using rapid transfusion devices such as a Level One or Bellmont however is still important for EMS. A 14g with a pressure bag can infuse 1L of fluid is under 2 minutes. Also great for blood products. Depending on length some 14g catheters actually flow faster than a Cordis.
/https://lifeinthefastlane.com/ccc/device-flow-rates/
https://etmcourse.com/large-bore-iv-access-showdown/
For large volume rapid infusion short/wide PIV catheters are best. As you can see from the chart length makes a big difference in IVs of the same gauge (Poiseuille's Law). IOs and CVC are great for medications but worthless for rapid infusion. Pressure bags or just squeezing the bag can increase flow rates substantially.
The biggest thing that many people do not realize is how much flow rates are decreased with needless connectors or extension sets. As much as 30-40% less. If you need high flow connect tubing directly to the catheter hub. It is hard to break the habit of instantly putting a saline lock and the IV you just placed.
If you only have the one IV and you are frequently pushing medications then a 3-way stopcock is a good compromise. Stopcocks will restrict flow slightly but much less than a needless connector. If you happen to see a stopcock with a yellow top then those are usually "High Flow" are will likely flow as fast as your IV will allow.
You can usually find these in the Cath Lab or with Anesthesia supplies.
So long story short Large Bore IVs are extremely useful when used appropriately. If you need high flow then go for a 14g or 16g, ditch the needless connector, and grab a pressure bag.