Hockey
Quackers
- 1,222
- 6
- 38
I consider myself decent with 12 leads and I am always looking to learn something I may miss or don't know
This is one I had the other night.
Called for shortness of breath at like 430 in the morning at a nursing home.
85ish year old female. Recent CVA in July. Had shortness of breath about 40 minutes ago, nursing home gave a breathing treatment and took care of patients shortness of breath problem. No more wheezing. Patient has no complaints other than chronic back pain.
Hx: Hypertension, Diabetic II, CVA July with left sided deficits. No cardiac history besides hypertension. No lung problems other than "seasonal allergies".
The nursing home just got the patient about 24 hours prior. Nurse was useless as usual.
Lung sounds clear.
BP 152/98
HR 110-130
Resp 24
Pupils fine
Denies chest, head, neck and back pain.
Denies any shortness of breath
AO x 3 or 4
No old 12 leads available.
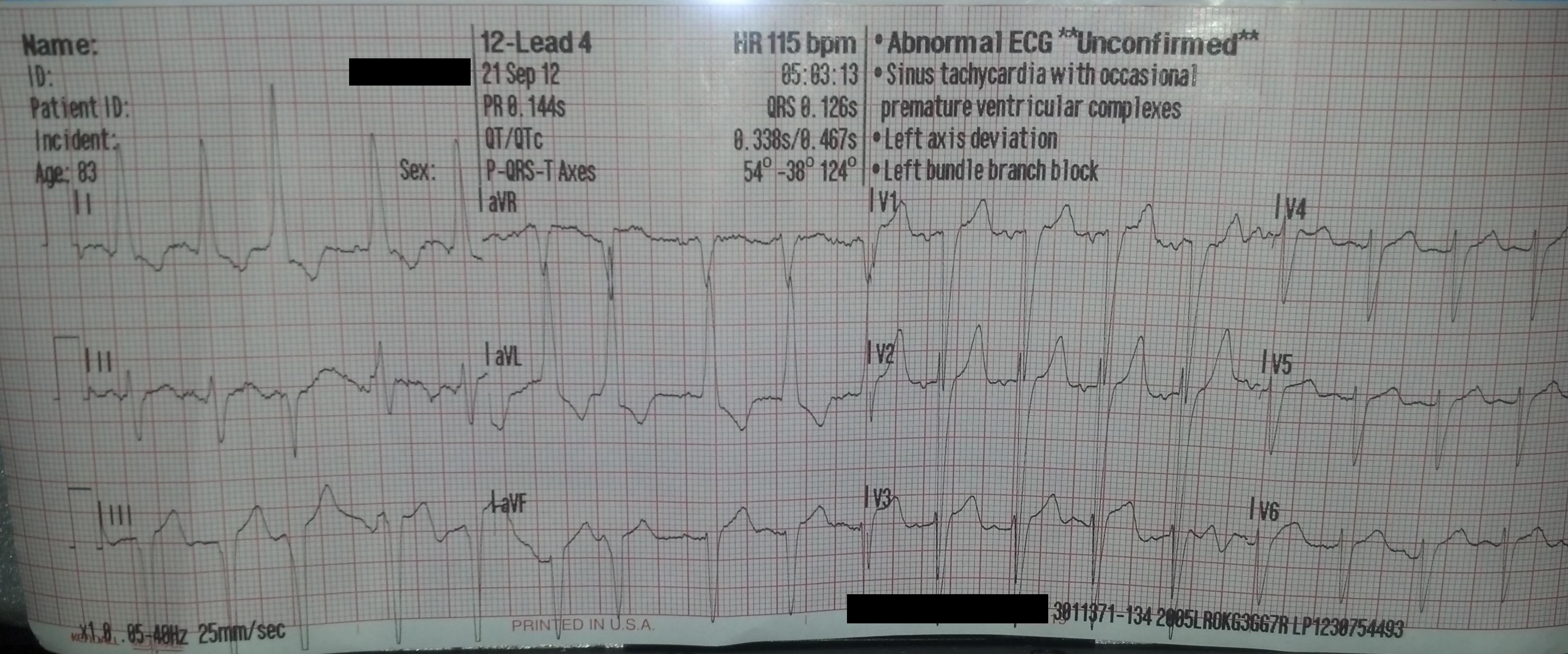
When we arrived at the hospital, the MD was waiting at the desk and I gave him a copy of the 12 lead. He decided since there was no old 12 lead available, and family was unable to be contacted, to activate a "Level II Acute MI"
Presence of left axis deviation. I see some elevation as well.
Just need to reassure some things about BBB's...when checking for BBB's, you look in V1 and if the QRS is greater than 120ms then it is, correct? I understand there should be a RsR wave in V6 but I don't see it here. Am I missing something?
What else do you see could be going on?
This is one I had the other night.
Called for shortness of breath at like 430 in the morning at a nursing home.
85ish year old female. Recent CVA in July. Had shortness of breath about 40 minutes ago, nursing home gave a breathing treatment and took care of patients shortness of breath problem. No more wheezing. Patient has no complaints other than chronic back pain.
Hx: Hypertension, Diabetic II, CVA July with left sided deficits. No cardiac history besides hypertension. No lung problems other than "seasonal allergies".
The nursing home just got the patient about 24 hours prior. Nurse was useless as usual.
Lung sounds clear.
BP 152/98
HR 110-130
Resp 24
Pupils fine
Denies chest, head, neck and back pain.
Denies any shortness of breath
AO x 3 or 4
No old 12 leads available.
When we arrived at the hospital, the MD was waiting at the desk and I gave him a copy of the 12 lead. He decided since there was no old 12 lead available, and family was unable to be contacted, to activate a "Level II Acute MI"
Presence of left axis deviation. I see some elevation as well.
Just need to reassure some things about BBB's...when checking for BBB's, you look in V1 and if the QRS is greater than 120ms then it is, correct? I understand there should be a RsR wave in V6 but I don't see it here. Am I missing something?
What else do you see could be going on?
Last edited by a moderator:
