tpchristifulli
Forum Crew Member
- 36
- 16
- 8
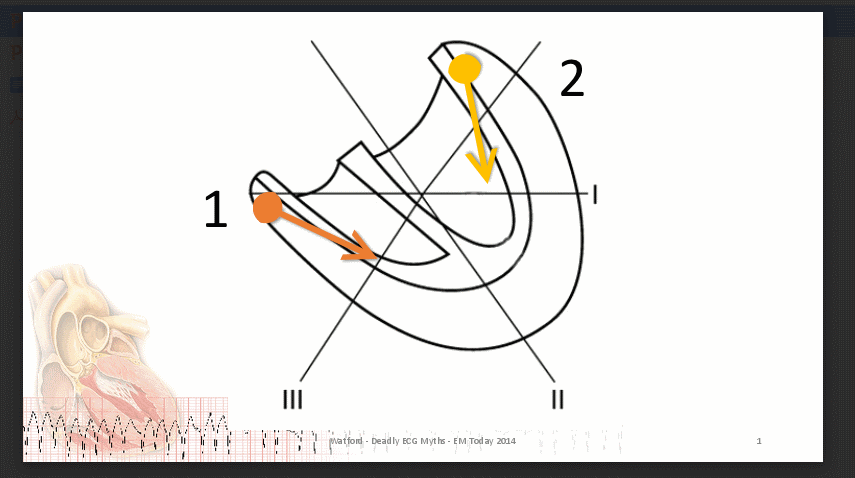
I was reviewing axis deviation today and wondered why Vtach is commonly ruled out if axis isn't extreme right. I would think that this would have to depend on where the focus is originating and the direction it depolarizes. Does vtach always depolarize towards the SA node or right side of the heart? If the focus depolarizes toward the left ventricle wouldn't lead 1 be mostly positive? What's your thoughts?