@ systemet, good interpretation you have been studying lately and i like that.
Sort of. I've been out of the field for a couple of years, going to school. Now I'm thinking about going back to working as a paramedic in a year. It seemed like a good idea to start reviewing things before that!
")
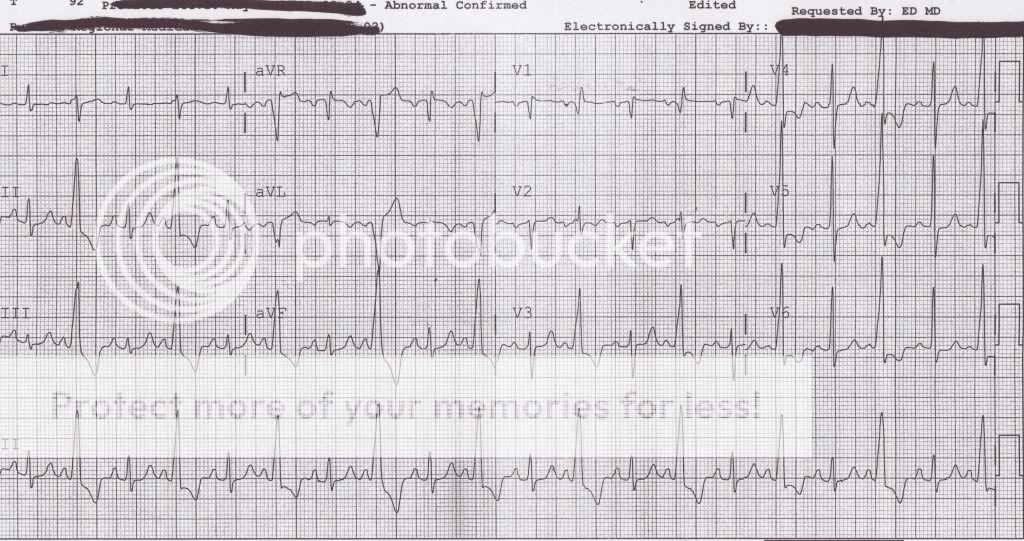
however i have one question, maby i missed it, but how are you explaining the the P-waves in front of your "PVC".
P waves arise (probably in the ventricles), transmit to the AV node, and undergo AV delay. Around the same time, an ectopic focus in the ventricles fires, creating a PVC. The SA-initiated depolarisation never passes the AV node, the impulse that originates in the ventricles depolarises them, but is blocked from (retrogradely) propagating into the atria by the AV node.
So we see the P wave, as the atria depolarise, but the wide complex that follows originates from an ectopic ventricular focus.
I think in this case leaving it as Bundle conduction delay would be more appropriate than trying to truly define it.
It might be. It's a possibility. Distinguishing ventricular complexes / rhythms from aberrantly conducted sinus/atrial/junctional rhythms is difficult.
what we have is a wide complex rhythm which came after V-FIB and V-TACH yea the 12 lead is not going to be normal after that... wait 30min to an hour and see what it is then i guarantee it will be different.
I thought this was a new patient? Is this the same patient from the previous ECGs?
This is still a sinus rhythm.
If this is a post-arrest ECG, I agree, there's a good chance it will look different in a while. Treating arrhythmias in the post-arrest period can often cause more problems than it fixes. Without knowing the clinical state of the patient, it's impossible to decide on treatment.
here if you have a ventricular rhythm with ROSC you go to the cath lab, and i believe we have found occlusions in 100% of our patients meeting these requirements.
Really?
Perhaps I'm misunderstanding what you've written -- but it sounds like you're saying all of your patients with post-arrest VT have had coronary occlusions on angiography? Is this published anywhere? How many patients is 100%?
please i am not being a smart ***, but after an arrest there is going to be ischemic, and altered conduction. you have to take the 12 lead at face value and treat you patient.
Absolutely. I'm not trying to be a d**k either. I agree post-arrest 12-leads may show ischemic changes. I also get that changes on the ECG need to be evaluated on the basis of the patient's clinical condition.
I realise I'm a little rusty, but I do have a little experience. This isn't my first walk in the park
")
notice: please disregard any spelling or grammatical errors i dont feel like editing right not
No problem. Please do the same!