Chief Complaint
Forum Captain
- 429
- 1
- 0
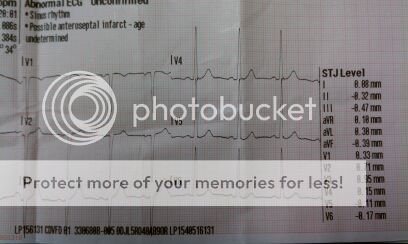
Just wanted some of your input as to what is going on in this ECG. Doing some LP 15 training and this is part of the strip taken from a coworker. I didnt snap a pic of the entire strip because i figured it would be too hard to see any detail in such a small pic. Can provide it if needed though.
Interpretation by the LP 15 is possible anteroseptal infarct. My coworker is a healthy 31 year old male. Is there such a thing as benign ST elevation? Not sure what to make of this.
Interpretation by the LP 15 is possible anteroseptal infarct. My coworker is a healthy 31 year old male. Is there such a thing as benign ST elevation? Not sure what to make of this.