Christopher
Forum Deputy Chief
- 1,344
- 74
- 48
Here is an interesting case which came across my desk that I'd like to share, the full details of which will be in a post on my blog shortly:
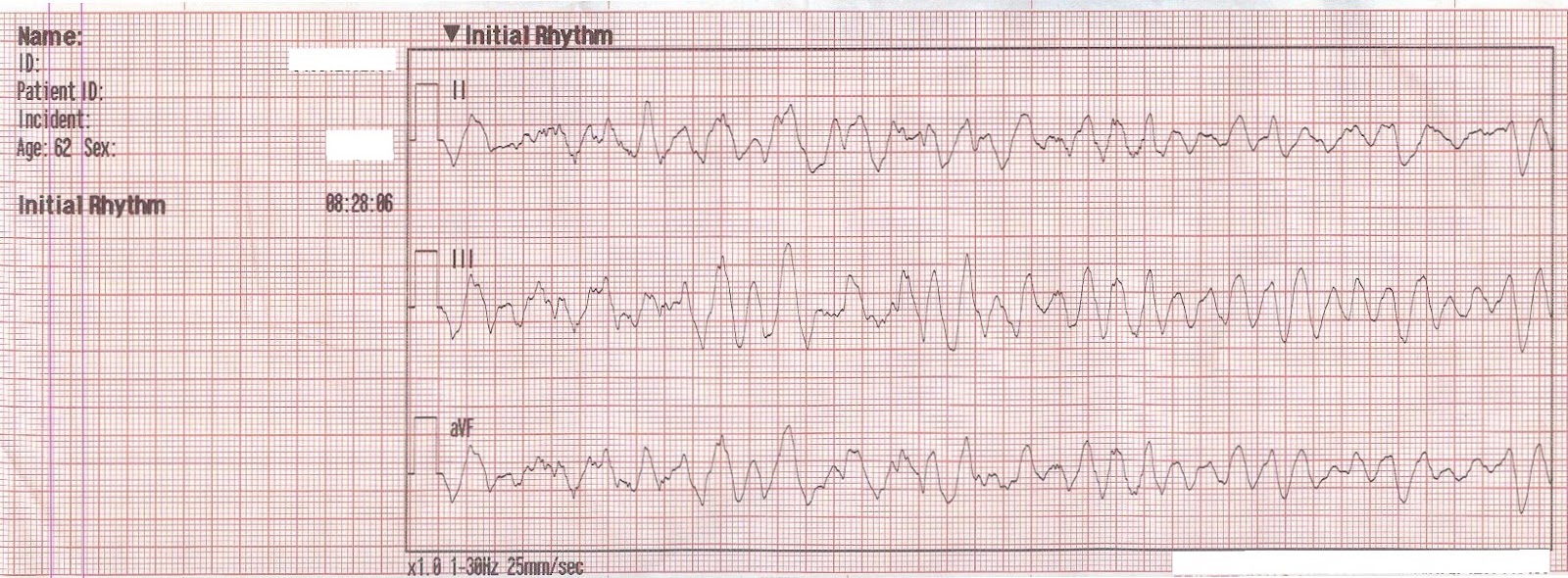
Printed summary of synchronized cardioversion (click for mega-res):

So what do you think happened next?
EMS was dispatched for a 62 year old male with an altered mental status. Upon their arrival they found the patient to be non-communicative, responsive to verbal stimuli, in moderate respiratory distress, with pale, diaphoretic skin, and weakly palpable radial pulses.
A 12-Lead ECG was obtained, showing a wide complex tachycardia with left axis deviation. It was interpreted by the paramedic as Ventricular Tachycardia.
A blood pressure was unobtainable, however a pulse of 150 was palpable at the carotid. Labored respirations were present, with clear breath sounds bilaterally. The patient had an extensive cardiac history, renal failure, and insulin dependent diabetes mellitus. The patient's blood sugar was 300 mg/dL.
Given the presence of hemodynamic instability the patient was prepped for synchronized cardioversion. Combo-pads were placed anterio-laterally, the Sync button was pressed, and sync markers were noted with each QRS complex.
Printed summary of synchronized cardioversion (click for mega-res):

So what do you think happened next?
")