medicRob
Forum Deputy Chief
- 1,754
- 3
- 0
Prehospital Intravenous Fluid Administration is Associated With
Higher Mortality in Trauma Patients: A National Trauma Data
Bank Analysis
Objective: Prehospital intravenous (IV) fluid administration is common in trauma patients, although little evidence supports this practice. We hypothesized
that trauma patients who received prehospital IV fluids have higher
mortality than trauma patients who did not receive IV fluids in the prehospital
setting.
Methods: We performed a retrospective cohort study of patients from the
National Trauma Data Bank. Multiple logistic regression was used with
mortality as the primary outcome measure. We compared patients with versus
without prehospital IV fluid administration, using patient demographics,
mechanism, physiologic and anatomic injury severity, and other prehospital
procedures as covariates. Subset analysis was performed based on mechanism
(blunt/penetrating), hypotension, immediate surgery, severe head injury, and
injury severity score.
Results: A total of 776,734 patientswere studied.Approximately half (49.3%)
received prehospital IV. Overall mortality was 4.6%. Unadjusted mortality
was significantly higher in patients receiving prehospital IV fluids (4.8% vs.
4.5%, P < 0.001).Multivariable analysis demonstrated that patients receiving
IV fluids were significantly more likely to die (odds ratio [OR] 1.11, 95%
confidence interval [CI] 1.05–1.17). The associationwas identified in nearly all
subsets of trauma patients. It is especially marked in patients with penetrating
mechanism (OR 1.25, 95% CI 1.08–1.45), hypotension (OR 1.44, 95% CI
1.29–1.59), severe head injury (OR 1.34, 95% CI 1.17–1.54), and patients
undergoing immediate surgery (OR 1.35, 95% CI 1.22–1.50).
Conclusions: The harm associated with prehospital IV fluid administration
is significant for victims of trauma. The routine use of prehospital IV fluid
administration for all trauma patients should be discouraged.
Discussion:
There are several inherent flaws in this study, most of them related to flaws in the National Trauma Data Bank. The National Trauma Data Bank (NTDB) is a compilation of information regarding traumatic injuries and subsequent outcomes in the United States. Emergency rooms, trauma centers, and other institutions participate in data submission, and in return, these agencies are given access to reports analyzing data regarding their own oeprations as well as trauma medicine in the United States as a whole. Researchers are also granted access to the data sets on an approval basis.
The Problems
While this system is useful in a variety of circumstances, it is not entirely appropriate for prehospital research as it does not take into account factors such as, "Response Times", "ALS/BLS Response", and several other factors.
One flaw that can be readily identified in this study is that the National Trauma Data Bank (NTDB) makes no differentiation between when an IV is started and when fluid is administered. Furthermore, we are not told the amount of fluid that is administered to the patients. Moreover, we there is no specification as to which medics started an IV on scene and delayed transport or whether the IVs were started in transport.
These are some very important parameters missing for this type of study.. especially for a study which concludes, "The harm associated with prehospital IV fluid administration is significant for victims of trauma. The routine use of prehospital IV fluid administration for all trauma patients should be discouraged."1
Here is a list of flaws outlined by Roguemedic in his blog
Another interesting finding by Rogue Medic:
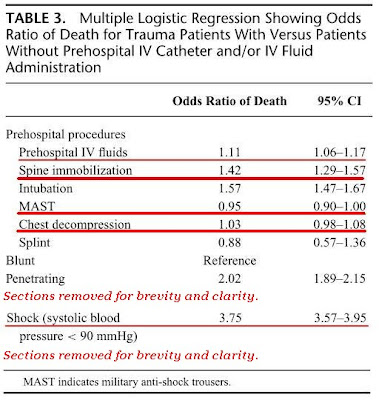
"Even though the authors concluded that IV Starts produced worse outcomes, the procedure most strongly correlated with IV Starts was determined to have produced a protective effect. Most IV Start patients had MAST applied, while less than one fifth of one percent of the No IV Start patients had MAST applied.
Intubation (OR 1.57) and spinal immobilization (OR 1.42) were found to increase the odds of death by much more than IV Starts (OR 1.11) were increasing the odds of death.
If these numbers were valid, the increased odds of death should result in strongly worded warning letters on the hazards of spinal immobilization and intubation of trauma patients."2
I invite each of you to check out Rogue Medic's analysis of this paper over on his blog. There are several good points made, some bad. However, the basic consensus of the prehospital research community with regard to this study is that the data provided cannot be relied upon to make a decision as to whether or not prehospital IV fluids increase mortality in trauma patients, due to what seems to be erroneous data entry in the NTDB, lack of important parameters such as delays caused by IV starts on scene, amounts of fluid administered, as well as transport times.
http://www.medicalscg.de/files/tccc_haut_prehospital_iv_fluids_ann_surg_2011.pdf
Link to RogueMedic's article:
Click Me.
References
1. Haut ER, Kalish BT, Cotton BA, Efron DT, Haider AH, Stevens KA, Kieninger AN, Cornwell EE, 3rd, Chang DC. Prehospital intravenous fluid administration is associated with higher mortality in trauma patients: A national trauma data bank analysis. Ann Surg. 2010
2. Rogue Medic. Prehospital fluid administration is associated with higher mortality in trauma patients (parts i - iii). Rogue Medic. 2011;2011
Higher Mortality in Trauma Patients: A National Trauma Data
Bank Analysis
Objective: Prehospital intravenous (IV) fluid administration is common in trauma patients, although little evidence supports this practice. We hypothesized
that trauma patients who received prehospital IV fluids have higher
mortality than trauma patients who did not receive IV fluids in the prehospital
setting.
Methods: We performed a retrospective cohort study of patients from the
National Trauma Data Bank. Multiple logistic regression was used with
mortality as the primary outcome measure. We compared patients with versus
without prehospital IV fluid administration, using patient demographics,
mechanism, physiologic and anatomic injury severity, and other prehospital
procedures as covariates. Subset analysis was performed based on mechanism
(blunt/penetrating), hypotension, immediate surgery, severe head injury, and
injury severity score.
Results: A total of 776,734 patientswere studied.Approximately half (49.3%)
received prehospital IV. Overall mortality was 4.6%. Unadjusted mortality
was significantly higher in patients receiving prehospital IV fluids (4.8% vs.
4.5%, P < 0.001).Multivariable analysis demonstrated that patients receiving
IV fluids were significantly more likely to die (odds ratio [OR] 1.11, 95%
confidence interval [CI] 1.05–1.17). The associationwas identified in nearly all
subsets of trauma patients. It is especially marked in patients with penetrating
mechanism (OR 1.25, 95% CI 1.08–1.45), hypotension (OR 1.44, 95% CI
1.29–1.59), severe head injury (OR 1.34, 95% CI 1.17–1.54), and patients
undergoing immediate surgery (OR 1.35, 95% CI 1.22–1.50).
Conclusions: The harm associated with prehospital IV fluid administration
is significant for victims of trauma. The routine use of prehospital IV fluid
administration for all trauma patients should be discouraged.
Discussion:
There are several inherent flaws in this study, most of them related to flaws in the National Trauma Data Bank. The National Trauma Data Bank (NTDB) is a compilation of information regarding traumatic injuries and subsequent outcomes in the United States. Emergency rooms, trauma centers, and other institutions participate in data submission, and in return, these agencies are given access to reports analyzing data regarding their own oeprations as well as trauma medicine in the United States as a whole. Researchers are also granted access to the data sets on an approval basis.
The Problems
While this system is useful in a variety of circumstances, it is not entirely appropriate for prehospital research as it does not take into account factors such as, "Response Times", "ALS/BLS Response", and several other factors.
One flaw that can be readily identified in this study is that the National Trauma Data Bank (NTDB) makes no differentiation between when an IV is started and when fluid is administered. Furthermore, we are not told the amount of fluid that is administered to the patients. Moreover, we there is no specification as to which medics started an IV on scene and delayed transport or whether the IVs were started in transport.
These are some very important parameters missing for this type of study.. especially for a study which concludes, "The harm associated with prehospital IV fluid administration is significant for victims of trauma. The routine use of prehospital IV fluid administration for all trauma patients should be discouraged."1
Here is a list of flaws outlined by Roguemedic in his blog
the mean systolic blood pressure of penetrating trauma patients who received cardiopulmonary resuscitation was 118 mmHg.
"That is higher than my blood pressure.
I am pretty sure that the AHA (American Heart Association) does not want anybody using CPR (CardioPulmonary Resuscitation) on people with good blood pressures. CPR is for people with no blood pressure (or for children with extremely low blood pressures).
Does this give us a hint about the reliability of the information used?
I think so."2
Another interesting finding by Rogue Medic:
"Even though the authors concluded that IV Starts produced worse outcomes, the procedure most strongly correlated with IV Starts was determined to have produced a protective effect. Most IV Start patients had MAST applied, while less than one fifth of one percent of the No IV Start patients had MAST applied.
Intubation (OR 1.57) and spinal immobilization (OR 1.42) were found to increase the odds of death by much more than IV Starts (OR 1.11) were increasing the odds of death.
If these numbers were valid, the increased odds of death should result in strongly worded warning letters on the hazards of spinal immobilization and intubation of trauma patients."2
I invite each of you to check out Rogue Medic's analysis of this paper over on his blog. There are several good points made, some bad. However, the basic consensus of the prehospital research community with regard to this study is that the data provided cannot be relied upon to make a decision as to whether or not prehospital IV fluids increase mortality in trauma patients, due to what seems to be erroneous data entry in the NTDB, lack of important parameters such as delays caused by IV starts on scene, amounts of fluid administered, as well as transport times.
http://www.medicalscg.de/files/tccc_haut_prehospital_iv_fluids_ann_surg_2011.pdf
Link to RogueMedic's article:
Click Me.
References
1. Haut ER, Kalish BT, Cotton BA, Efron DT, Haider AH, Stevens KA, Kieninger AN, Cornwell EE, 3rd, Chang DC. Prehospital intravenous fluid administration is associated with higher mortality in trauma patients: A national trauma data bank analysis. Ann Surg. 2010
2. Rogue Medic. Prehospital fluid administration is associated with higher mortality in trauma patients (parts i - iii). Rogue Medic. 2011;2011
Last edited by a moderator: